

Introduction: Haploidentical donor transplant (HIDT) with high dose post-transplant cyclophosphamide (PTcy) has shown promising results in terms of GVHD and survival. PTcy when given on day +3 and +4 is associated with considerable morbidity. In our previous analysis, we demonstrated that when compared to matched donor allogeneic stem cell transplant, HIDT with PTcy was associated with significantly higher rates of hypoxia, grade 3-4 mucositis and hemorrhagic cystitis (Modi et al, JCO 2020). PTcy is known to cause cardiomyopathy. However, a comprehensive analysis of cardiac toxicity occurring from PTcy is limited.
Methods: We retrospectively evaluated adult patients (pt) who underwent HIDT with PTcy to evaluate incidence and risk factors of cardiac toxicities. Source of stem cell was peripheral blood in all patients, and all received PTcy-based GVHD prophylaxis. We aimed to evaluate impact of cardiac toxicity on NRM and OS. We compared outcomes between two groups: cardiac toxicity and no-cardiac toxicity.
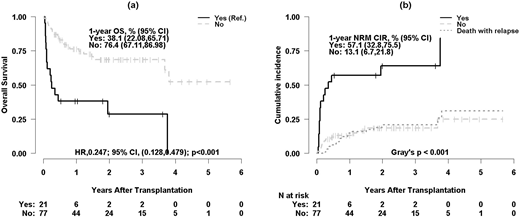
Results: Between June 2012 and June 2019, 98 pt underwent HIDT. Of these, 21 (21.4%) developed cardiac toxicity and 77 (78.6%) did not. Median day to onset of cardiac toxicity from HIDT was 7 days, and median duration of cardiac toxicity was 14 days. Fourteen pt (67%) had resolution of the cardiac toxicity. Median age of the patient was significantly higher in the cardiac toxicity than no-cardiac toxicity (65 vs 57 years, p=0.007). Following cardiac toxicities were observed: systolic heart failure (n=7, 34%), diastolic heart failure (n=2, 10%), atrial fibrillation (n=10, 48%), pericardial effusion (n=2, 9%) one of which required pericardial window, pericarditis (n=1, 5%) and supraventricular tachycardia (n=1, 5%). In patients with congestive heart failure, the median LVEF was 45% (range, 20-60). Majority of the cardiac toxicities were de-novo in origin, while sepsis-induced cardiac toxicity was present in one pt. The proportion of male patients was higher in the cardiac toxicity than no-cardiac toxicity (81% vs 55%, p=0.04). Median KPS was marginally lower (70% vs 80%, p=0.08) and median donor age was marginally higher (59 vs 51 years, p=0.08) in the cardiac toxicity group compared to no-cardiac toxicity. Median Co-morbidity index was 1 for both groups. Patients in the cardiac toxicity had higher rate of pre-transplant coronary artery disease compare to no-cardiac toxicity group (24% vs 6%, p=0.03). No difference in the pre-transplant cardiac function was noted between both groups (LVEF 55% vs 60%, p=0.76). Six pt (29%) in the cardiac toxicity and 30 pt (39%) in the no-cardiac toxicity received myeloablative conditioning regimen (p=0.45). Grade 3-4 cytokine release syndrome was higher in the cardiac toxicity compared to the other group (20% vs 6%, p=0.04). Median follow-up of surviving patients was 1.9 years in both groups. For cardiac toxicity and no-cardiac toxicity, 1-year OS was 38.1% and 76.4% (HR 0.25, 95% CI 0.13-0.48, p≤0.001), respectively; and 1-year NRM was 57.1% and 13.1%, respectively (P≤0.001). Multivariable analysis was performed to evaluate risk factors associated with cardiac toxicity, and older age (OR 1.05, 95% CI 1.00-1.10, p=0.08) and male sex (OR 0.34, 95% CI 0.08-1.13, p=0.096) were marginally associated with higher risk of cardiac toxicity. No impact of intensity of conditioning regimen was noted. Multivariable analysis revealed adverse OS (HR 0.20, 95% CI 0.09-0.43, p<0.001) and significantly higher NRM (SHR 0.19, 95% CI 0.09-0.40, p<0.001) in patients with cardiac toxicity than the other group.
Conclusion: Cardiac toxicity was associated with worse OS and higher NRM. Older age and male sex may have higher risk of developing cardiac toxicity. Early supportive care and aggressive cardiac management may help improve outcomes.
Deol:Kite, a Gilead Company: Consultancy; Novartis: Consultancy. Modi:MorphoSys: Membership on an entity's Board of Directors or advisory committees.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal